A comprehensive SOAP note has to take into account all subjective and objective information, and accurately assess it to create the patient-specific assessment and plan.
How do you write a comprehensive SOAP note?
- Find the appropriate time to write SOAP notes.
- Maintain a professional voice.
- Avoid overly wordy phrasing.
- Avoid biased overly positive or negative phrasing.
- Be specific and concise.
- Avoid overly subjective statement without evidence.
- Avoid pronoun confusion.
- Be accurate but nonjudgmental.
What is the purpose of SOAP notes?
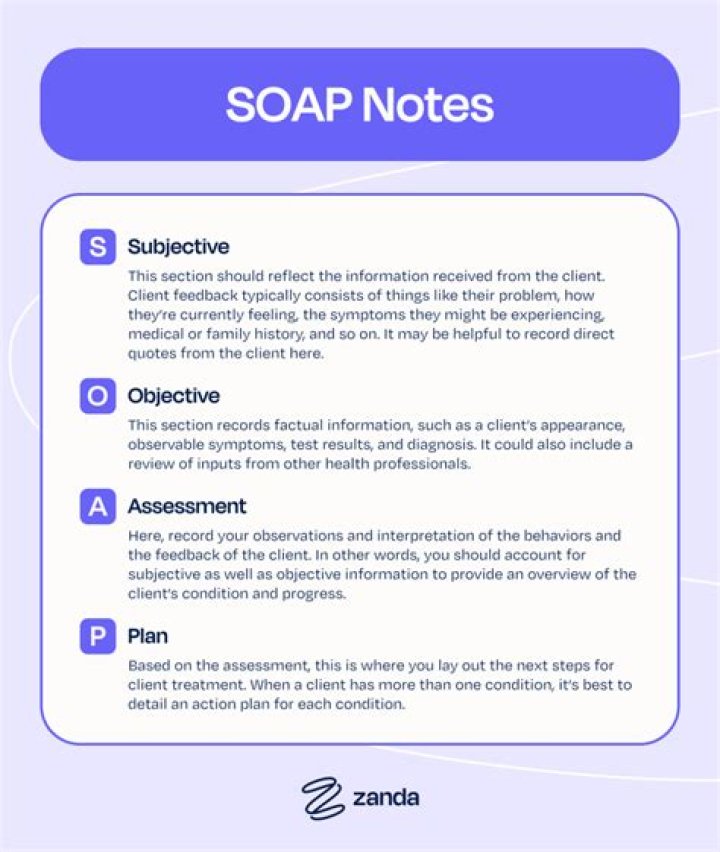
Today, the SOAP note – an acronym for Subjective, Objective, Assessment, and Plan – is the most common method of documentation used by providers to input notes into patients’ medical records. They allow providers to record and share information in a universal, systematic and easy-to-read format.
What is included in a SOAP note?
A SOAP note is a form of written documentation many healthcare professions use to record a patient or client interaction. … However, all SOAP notes should include Subjective, Objective, Assessment, and Plan sections, hence the acronym SOAP.What is a more detailed SOAP note called?
A SOAP note also known as. A “Progress note”
What do the two Ds in Cheddar stand for?
What do the two Ds in CHEDDAR stand for? details and drugs.
Where are labs in SOAP notes?
Results of diagnostic tests, such as lab work and x-rays can also be reported in the objective section of the SOAP notes.
What does the receiver do to decode messages?
Decoding is conducted by the receiver. … The receiver begins to interpret the symbols sent by the sender, translating the message to their own set of experiences in order to make the symbols meaningful. Successful communication takes place when the receiver correctly interprets the sender’s message.What does acronym SOAP stand for?
The Subjective, Objective, Assessment and Plan (SOAP) note is an acronym representing a widely used method of documentation for healthcare providers. The SOAP note is a way for healthcare workers to document in a structured and organized way.[1][2][3]
What does the P in soap stand for quizlet?What does SOAP stand for? S=Subjective (something patient tells you) O=Objective (something clinician does to patient) A=Assessment (Putting info together, and figure out what it means) P=Plan (how to get the patient to their highest lvl of function)
Article first time published onWhat does the C represent in the cheddar method of progress notes?
CHEDDAR Format – CHEDDAR stands for chief complaint, history, examination, details, drugs and dosages, assessment, and return visit.
What does the P stand for in POMR?
PROBLEM-ORIENTED MEDICAL RECORD (POMR)
Why is it important to completely remove a file from the drawer in order to file correctly?
Why is it important to completely remove a file from the drawer in order to file correctly? *If not done, it could lead to misfiling.
Which of the following is not a covered entity under Hipaa?
Under HIPAA, which of the following is not considered a provider entity: Business associates. Us Healthcare entities are outsourcing certain services such as Transportation to foreign country. Offshore vendors are not covered and see under HIPAA and do not have to comply with HIPAA privacy and security legislation.
What are SOAP notes in counseling?
SOAP notes are the way you document that a client participated in and completed a session with you. Depending on the billing process you have, a completed therapy note may also be the way a claim is generated. Documentation also demonstrates your competency and shows how a client’s needs have been addressed.
What are the 2 most common Assistant level jobs?
what are the two most common assistant level jobs? Nurse and medical assistants.
What is the difference between decoder and receiver?
On the other hand, Decoding is the process in which the encoded message is interpreted or understood to fulfil the purpose of communication. The receiver is the decoder who translates the coded message into an understandable form. Decoding depends on the type of message that is being sent.
Who is the decoder of ad messages?
The decoding of a message is how an audience member is able to understand, and interpret the message. It is a process of interpretation and translation of coded information into a comprehensible form.
What is the H in hops?
History, Observation, Palpation, Special Tests. What does the H mean in H.O.P.S. Involves asking questions to help determine the mechanism of injury to access the injury. You just studied 10 terms!
What does hops and soap stand for?
1. Differentiate between the history of the injury, observation and inspection, palpation, and special tests (HOPS) injury assessment format and the subjective evaluation, objective evaluation, assessment, and plan (SOAP) note format used to assess and manage musculoskeletal injuries.
What does the H in hops mean?
History, Observation, Palpation and Special Tests.
What are six types of patient files?
- PIL. A PIL is a patient information leaflet you can find in any medicine bought at a pharmacy. …
- Medical history record. …
- Discharge Summary. …
- Medical test. …
- Mental Status Examination. …
- Operative Report.
Who is the owner of a health record?
Your physical health records belong to your health care provider, but the information in it belongs to you. Having ownership and control over that information helps you ensure that your personal medical records are correct and complete.
What are the Six C's of charting?
The Six C’s of Medical Records Client’s Words, Clarity, Completeness, Conciseness, Chronological Order and Confidentiality. Client’s Words – a medical assistant should always record the patient’s exact words.
What are the disadvantages of POMR?
As a patient-focused approach, POMR is advantageous to both patients and providers. The problem is that many doctors avoid using it, arguing that it’s too cumbersome, has many data synthesis restrictions and requires one to take a lot of notes.
Why is the POMR system commonly used by family practice clinics?
POMR associates a problem source with a number per visit. Used for general medicine because they see their patients more often and longer.
What is one of the main differences between the POMR and the SOMR?
Describe the difference between a POMR and the SOMR? POMR list the list of the patient’s problems in numerical order the SOMR is the organized source in the chart of patient’s medical record. Component of the patient’s medical history record is when the patient describes in his own words the reason for the visit?